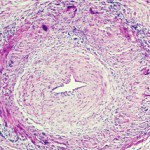
Although scientists characterize giant cell arteritis (GCA) as an immune-mediated disease, its cause is unknown. A new study by Don Gilden, MD, and Maria Nagel, MD, of the University of Colorado School of Medicine in Aurora, Colo., suggests that an infection with the varicella zoster virus (VZV) may trigger GCA. The neurologists published their analysis of temporal arteries (TAs) in a supplement of the Journal of Infectious Diseases.1
Although scientists characterize giant cell arteritis (GCA) as an immune-mediated disease, its cause is unknown. A new study by Don Gilden, MD, and Maria Nagel, MD, of the University of Colorado School of Medicine in Aurora, Colo., suggests that an infection with the varicella zoster virus (VZV) may trigger GCA. The neurologists published their analysis of temporal arteries (TAs) in a supplement of the Journal of Infectious Diseases.1
VZV is a neurotropic virus found exclusively in humans. After causing chicken pox, the virus becomes latent in cranial nerve ganglia, dorsal root ganglia and autonomic ganglia along the entire neuroaxis. In elderly and immunocompromised individuals, VZV-specific, cell-mediated immunity declines and VZV reactivates from one or more ganglia. The reactivation results in a productive viral infection that can cause shingles. Shingles may also be complicated by VZV vasculopathy when the viral infection includes the cerebral arteries.